
Understanding the connection between hip mobility, adductor strength, and pelvic floor function is essential for achieving lasting rehabilitation outcomes in pelvic health patients.
Why Your Pelvic Floor Patients Need Hip and Adductor Work
In the clinic, it’s easy to silo the pelvic floor. A patient presents with pelvic pain, urgency, or dyspareunia, and the reflex is to zoom in locally. But clinically — and mechanically — the pelvic floor rarely behaves like an isolated structure. It functions more like a hub in a broader myofascial and neuromuscular system.
When we step back and look through a whole-body lens (very much in line with Institute of Physical Art thinking), we often find that persistent pelvic floor tone is being driven from the hips and surrounding musculature.
Recently, at our in-person Bay Area study group, we spent time working through exactly this concept — palpating adductors, assessing hip rotation control, and discussing how often medial thigh tone mirrors pelvic floor overactivity. I’ve included a short video from that session below so you can see how we’re thinking about screening and integrating this clinically.
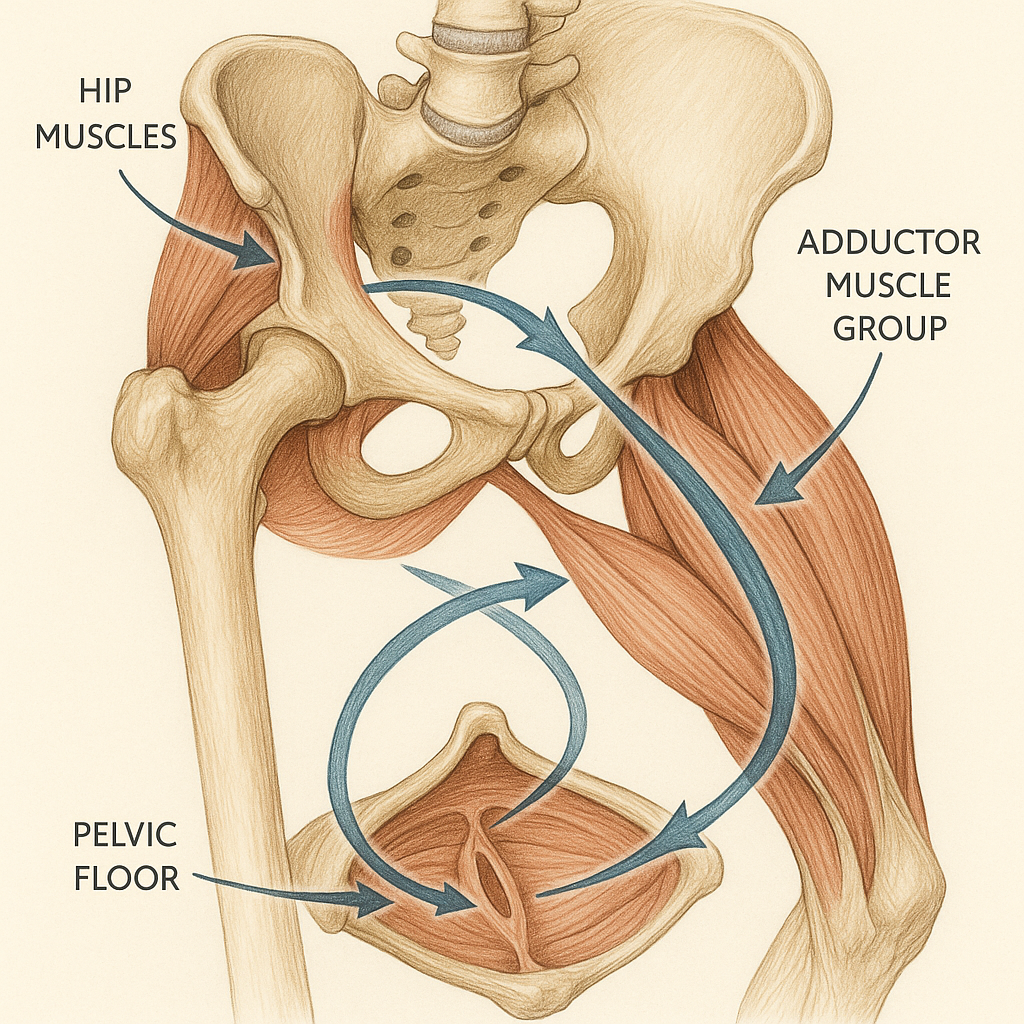
The Hip–Pelvic Floor Relationship
The adductors, obturator internus, hamstrings, and gluteal complex share dense fascial and neuromotor relationships with the pelvic floor. In practice, many patients with pelvic floor overactivity present with increased tone or guarding in the adductor group and deep hip rotators.
From a mechanical and motor control perspective, this makes sense. The body is constantly seeking balanced tension — tensegrity. When load or control is altered at the hips, the pelvic floor often becomes a compensatory stabilizer.
Treating the pelvic floor without addressing these contributors can leave the true driver of the problem untouched.
A Simple (and Often Overlooked) Screen
Clinically, one of the simplest and most revealing screens is careful palpation of the adductor complex.
- Compare tone side-to-side.
- Note symptom reproduction.
- Observe how the tissue responds to gentle loading or release.
If the adductors are significantly guarded, it is often worth assuming that the obturator internus and related pelvic floor tissues are also contributing. This is not about treating everything everywhere — it’s about following the mechanical and neuromuscular clues the body gives us.
At the Bay Area study group, what stood out was how consistently medial thigh tone shifted once hip control strategies were addressed. When clinicians feel that change in real time, it reinforces how integrated this system truly is.
Don’t Skip the Posterior Chain
A second practical step is to broaden your posterior chain assessment. Quick screens of:
- Hamstring tone
- Glute activation patterns
- Hip rotation control
can reveal why the pelvic floor may be overworking.
In the IPA framework, we’re always asking:
Where is the system losing efficiency?
Where is the body creating protective tone to compensate?
Pelvic floor overactivity frequently reflects a regional strategy rather than a purely local problem.
Clinical Take-Homes
- Screen the adductors in every pelvic floor patient — tone and symptom reproduction matter.
- Consider obturator internus involvement when the medial thigh is reactive.
- Look at the posterior chain and hip control before assuming the problem is purely pelvic.
- Think system, not sling.
When we treat the pelvic floor as part of an integrated system rather than an isolated structure, outcomes tend to improve — and often more quickly than expected.
If you haven’t already, watch the video from our Bay Area study group above. It’s one thing to read about integration — it’s another to see and feel how quickly the system responds when you address the hips.